
Cath Labs
Forging ahead to new heights
The cath lab equipment industry is poised for exciting times ahead. Issues as after-sale-service being too expensive and the need to standardize safety and training practices for cardiac cath lab personnel however remain.

With the postponement of non-essential elective surgeries and medical procedures in COVID-stricken 2020, cardiovascular procedures took a backseat. The increased costs of caring for COVID patients, personal protective equipment (PPE), and the loss of elective procedure revenue caused a massive financial burden on healthcare providers. This is expected to result in reduced capital expenditure budgets for imaging equipment, including interventional angiography imaging systems and surgical mobile C-arm X-ray systems.
The global markets are estimated to have declined by 17.4 percent for cath lab angiography systems and 16.3 percent for surgical mobile C-arms in 2020, according to Signify Research. And expected to reach almost USD 3.9 billion by 2024. However, growth in this market is predicted to return from 2021 onwards, as the negative impact of the pandemic subsides. With the steady return of elective procedures and as healthcare expenditure is restored from the diversion to COVID-related equipment recovery is expected to be gradual rather than V shaped.
Mergers and acquisitions, partnerships, technology collaborations, and FDA and CE clearances are the key strategies followed by the players. In April 2021, Abbott received European CE mark and Health Canada authorization for its next-generation TriClip Transcatheter Tricuspid Valve Repair (TTVR) System, a minimally invasive tricuspid heart valve repair device to treat tricuspid regurgitation (TR). The same month, Philips Healthcare received USFDA 510(k) clearance for its SmartCT application software,a component of Philips Azurion Image Guided Therapy System. In December 2020, GE Healthcare had introduced a new version of its robotic driven angiography system for image guided therapy, the Allia IGS 7 angiography system. And in June 2020, Sahajanand Medical Technologies Pvt. Ltd acquired structural heart medical device firm Vascular Concepts.
There was a significant reduction in the functioning of the cardiac cath labs when compared to the previous functioning laboratories, due to the COVID-19 lockdown hampering the management of cardiac patients requiring indicated interventions. The maximum reduction was seen in diagnostic coronary angiography, and elective angioplasty. There was an increase in rescue angioplasty during the lockdown phase, but a fall in admissions of acute coronary syndrome and in heart failure admissions during the lockdown period. This resulted in less spend on the new cath labs too.
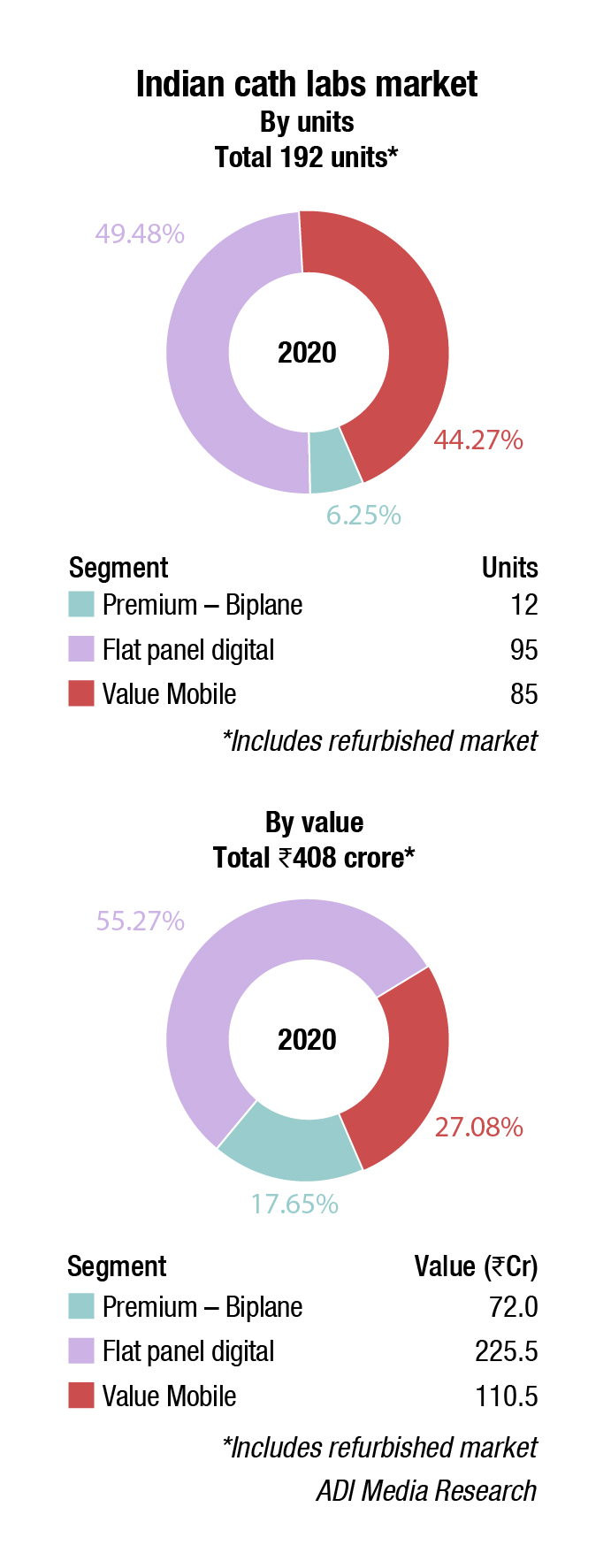
India has about 1600 cath labs in 140 cities. And 225 labs are added every year, albeit 2020 only saw 192 additions. With it being recognised that cardiovascular disease is not only an urban phenomenon, the medical facilities in tier 3 and 4 cities are also seeking to set up cath labs at Rs. 6-7 crore each. For instance, Punjab state government has only two cath labs, the government medical colleges of Amritsar and Faridkot. In the absence of cath labs, cardiac patients have to either pay around Rs.150,000 per angioplasty at private hospitals or travel to PGIMER Chandigarh. And many do not make it. The government will need to step up here.
| Tier I | Tier II | Others |
|---|---|---|
| Philips, GE, and Siemens | Allengers | Shimadzu, Schiller, Zhiem, Skanray, Toshiba, and IITPL |
| *Vendors are placed in different tiers on the basis of their sales contribution to the overall revenues of the Indian Indian cath lab market. | ||
| ADI Media Research | ||
World-class cath labs are being set up by the private hospitals. In October 2020, Fortis Hospital, Bengaluru installed one of the most modern biplane cath labs. The cath lab enables the surgeon to see blood vessels of the brain simultaneously in two different planes, the macine is capable of capable of extremely fast 3D acquisition of angiograms and CT scan inside the cath lab, and emergency neuro-interventional cases can now be treated with more precision.
India is the worldwide capital for diabetes and heart disease. It is no surprise that the need and demand for cardiac services and equipment continues to rise. A cardiac catheterization laboratory is an integral part of any contemporary large cardiology service. With increasing longevity and percutaneous solutions for several cardiac problems, the utilization of cardiac catheterization services in India is expected to rise even further.
With advent of newer procedures like TAVR, mitral clipping, and left atrial appendage occlusion the existing labs are also looking to upgrade and improve imaging quality, while minimizing radiation dosages. Labs integrated with intravascular ultrasound (IVUS), optical coherence tomography (OCT), laser systems, and superimposition of CT and TEE images on the cath lab images will start gaining steam.
There have been tremendous advancements in the field of interventional cardiology since the first coronary intervention was performed, over 40 years ago. From balloon catheters to guidewires to the blood thinners we use, these advances are nothing short of extraordinary. But despite these improvements, the fundamental technique used to perform percutaneous coronary intervention (PCI) has not changed and too often is guided only by a shadowy angiogram.
In recent years, intravascular ultrasound (IVUS) and optical coherence tomography (OCT) have been developed and improved as both diagnostic and guidance tools for interventional procedures. The development and improvement in intracoronary imaging technology represent a significant advancement in PCI technique. OCT, in particular, with its powerful platform, provides operators with a tremendous amount of information very rapidly in a user-friendly format. Nevertheless, despite clearly demonstrated benefits in multiple clinical trials, the utilization of intracoronary imaging remains low.
Although both, IVUS and OCT have many similarities, it remains controversial which intravascular imaging modality is better, and must be used as a diagnostic and guidance tool. Multimodality invasive imaging assessments are not recommended due to the increased risk of complications and cost. Technicians need to be aware of each modality’s advantages and disadvantages and select the imaging tool based on the clinical need, location of the segment of interest, angiographic appearance of the vessel, lesion characteristics, and operators’ experiences. In fact, a recent web-based survey suggested that most operators thought to use each imaging modality (IVUS and OCT) properly depended on the specific anatomic and patient characteristics.
One of the instances when OCT has limitations is at the time of blood clearance during pull-back, since the light signal is attenuated by the red blood cells. Blood clearance is achieved by contrast injection. The total volume of the contrast medium tends to be higher in OCT-guided PCI than those without OCT.
With respect to the imaging capabilities of intracoronary imaging, resolution and penetration depth are recognized as two important factors. OCT has the highest resolution among all the contemporary available coronary imaging modalities (axial 10–20 μm and lateral 20–90 μm), which is ~10 times greater than that of IVUS (axial 100–150 μm and lateral 150–300 μm). The higher resolution of OCT enables more detailed evaluation than IVUS at the endoluminal level and for the superficial plaque (e.g., in detecting cavity formation of a plaque rupture, TCFA, and stent architecture). With regards to its diagnostic performance of functionally significant stenosis, OCT has a better accuracy than IVUS in non-left main stem lesions.
 Role of cath labs in the current scenario
Role of cath labs in the current scenario
Ashu Goyal
Director – Sales (Cath Lab & CT),
Allengers Medical Systems Ltd
Cardiovascular disease has become a big challenge and has taken the shape of a national epidemic. Earlier it was presumed to be a disease of the elite class, but lately has become a common man’s disease. Thus, instead of being a product for the elite care segment, it is now considered as value-care one, as demand is arising not only from tier I, but from tier III as well. Meaning from urban to rural, no one is 100 percent secure, as the rural population is equally affected by to a cardiac diseases.
This is because of degradation to a sedentary lifestyle of the masses, increase in diabetes burden and pollution, which has further escalated cardiac diseases to a very large extent, be it any class.
So, today be it any topographic region, there is a huge demand for cath lab centers where a variety of interventional and diagnostic procedures are carried out for the treatment of CAD and other associated diseases.
Earlier, there were increased costs associated with cath lab projects, but now the dynamics are fast changing. Due to the emergence of Indian brands that provide all variants of cath labs from entry level to ceiling suspended models, there is a cath lab available for any tier or budget.
The government price regulation on the stent costs and availability of interventional cardiologists have further lowered the financial burden and smoothened the functioning of cath labs, even in the smaller cities.
Cath labs are available from reputed Indian players, and come with a host of affordable high-end features like dose management, AI, stent enhancement software, and high rating tubes for more throughput, which totally add value to this emerging high demand segment.
If a center’s overall costs to run a cath room are manageable, then there is lot of room for such high-end cath labs without shelling out huge amount of money for similar cath labs, thus even saving on foreign exchange.
Being Atmanirbhar Bharat, not only by thought but by also installing indigenous cath labs made in India, encompasses all needs that would be required.
Even during the ongoing COVID pandemic, the indigenous cath labs are playing a great role in saving precious lives. So, it is more important to have cath labs that are affordable to buy, economically viable to run along-keeping international quality standards.
In contrast to IVUS, OCT has lower tissue penetration depth (1–2 mm) than IVUS (5–6 mm), leading to incomplete visualization of the vessel wall especially in large vessels, or in case of an increased plaque burden. In this context, IVUS enables assessment of the deeper layers of the vessel than OCT, including adventitia.
Several studies attempted to fuse IVUS and OCT images obtained by two different imaging catheters in a serial fashion and showed the synergistically high potential of multimodality imaging for the evaluation of plaque composition, but they also suggested the limitation to acquire strict co-registration images by separate two pullbacks. To fuse IVUS and OCT images with two separate acquisition, it is necessary to detect several landmarks such as side branches and calcifications. Thereafter, it also takes time and effort to combine the two imaging modalities into a single image, a fact that makes impossible the broad application of this approach in research. A hybrid IVUS–OCT catheter system is warranted to enable accurate online co-registration and fusion of high-quality images obtained by the two imaging probes during a single pull-back.
Despite the fact that many interventional cardiologists are aware of the potential prognostic and clinical value of intravascular imaging-guided PCI, the application of intravascular imaging is still low in recent clinical practice, especially in Western countries. According to a web-based survey, the most common reason for the underuse of intravascular imaging is its high cost (65.9%), followed by the prolongation of the diagnostic procedure or intervention (35.0%), albeit risk of complications (9.5%) and absence of established clinical value (8.3%). However, IVUS-guided PCI has been reported to contribute to the favorable incremental cost-effectiveness, compared to angiography-guided PCI in the dedicated economic analysis.
The hybrid catheter has a marginal incremental cost to build, relative to a single modality imaging catheter that would not greatly impact the overall cost-effectiveness of intravascular imaging. The consoles and patient interface modules have costs that are associated with supporting ultrasound electronics as well as the optical components for OCT, and thus have a more noticeable, yet still modest, incremental cost over single modality systems to provide this advanced dual modality imaging capability.
For the purpose of detecting a high-risk plaque, a recent LRP trial demonstrated the impact of a Lipid Core Burden Index derived from NIRS-IVUS on future cardiac events, which was independent of intravascular ultrasound plaque burden or minimum lumen area. Further clinical trials will be needed to compare the hybrid IVUS-OCT system vs. NIRS-IVUS in terms of the prognostic performance in patients at risk.
Although the routine use of intravascular imaging is not currently recommended, its use is expected to reduce events in complex PCI. Moreover, in the era of emerging novel pharmacotherapies, a meticulous evaluation of plaque morphology would be required to discriminate the potential population in need. The hybrid IVUS–OCT systems have the potential to assess plaque morphology and PCI results. IVUS or OCT-which should be used?—this question has been frequently repeated. The hybrid IVUS–OCT system could be the answer in the near future.
The worldwide pandemic caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has placed an enormous strain on the healthcare systems of the nations where it has spread widely, with specific implications on practice in the catheterization laboratory. These implications include how experts might modify practice for standard cardiac patients, those who are suspected to have COVID-19, and those with COVID-19.
At this time, to preserve hospital bed capacity, it would seem reasonable to avoid elective procedures on patients with significant comorbidities or in whom the expected length of stay is more than a couple of days or anticipated to require intensive care. Procedures as percutaneous coronary intervention for stable ischemic heart disease, endovascular intervention for iliofemoral disease in patients with claudication, and patent foramen ovale closure are highly likely to be deferred. Of course, case decisions would be individualized, taking into account the risk for COVID-19 exposure versus the risk for delay in diagnosis or therapy.
Consideration should be given to laboratory downsizing case volumes (e.g., deferral of elective cases) and/or shift-based allocation of staff members and physicians needed to operate the laboratory in anticipation of likely disruptions to staffing.
The vast majority of catheterization laboratories have either normal or positive ventilation systems and are not designed for infection isolation. Given the need for terminal cleaning, following procedures on patients with suspected or known COVID-19, this aspect will need to be considered.
These cases should be done at the end of the working day if possible. For known COVID-19-positive patients, restriction of cases to a dedicated laboratory may be of value.
Finally, as the pandemic progresses, there will be need to create avenues for reporting and collation of data and then methods for rapidly dispersing that information in order to better care for patients and to protect healthcare workers in the cath lab.
The short- and long-term effect that COVID-19 poses on both patients and healthcare workers alike remains unknown. As infection rates vary in different areas of the nation, staff should remain vigilant and not grow complacent in upholding assessment and screening protocols, and safety measures with proper PPE, for all COVID-19 positive and suspect patients. The mental and physical safety of staff during this time remains of great importance, as we are dealing with constant change and uncertainty. The role of the cath lab during COVID-19 remains vital, because this patient population holds a high prevalence of cardiovascular diseases and manifestations requiring the activation of the cath lab staff in order to provide timely interventions.
 Dr Keshava R
Dr Keshava R
Director Cardiology,
Fortis Hospital, Bangalore
“Cath labs have revolutionized cardiac care in entire world. They have changed in size shape and quality enormously in last two decades. Initial bi-plane cath labs are now seen rarely now and seen used in neuro interventional procedures. Mono plane cath labs and hybrid cath labs are order of the day. Flat panel and digital cath labs with large storage space are available in Tier III cities now. Cath labs that can be used with DSA are useful in lower limb peripheral and cerebral angiograms are needed in multispecialty hospitals. Integration of cath labs with IVUS, OCT, and FFR for co-registration are used in high volume centers, which are routinely doing complex chip interventions in cardiology. Hybrid cath labs are used in complex aortic aneurysms, TAVI, and abdominal aneurysm procedures. Rlectro physiology procedures bring a different dimension to cath lab needs where integration of images from CT scan into cath lab is needed to do complex 3D navigational procedures.”









